
Taser Oh In-custody Death Certificate 2001
Download original document:
Document text
Document text
This text is machine-read, and may contain errors. Check the original document to verify accuracy.
Reg. Dist No.
DO HOT WRITE 'N
MAIlG'N
Il{SfIlll£O 'OR DOH
Primary Reg. DiSl. No.
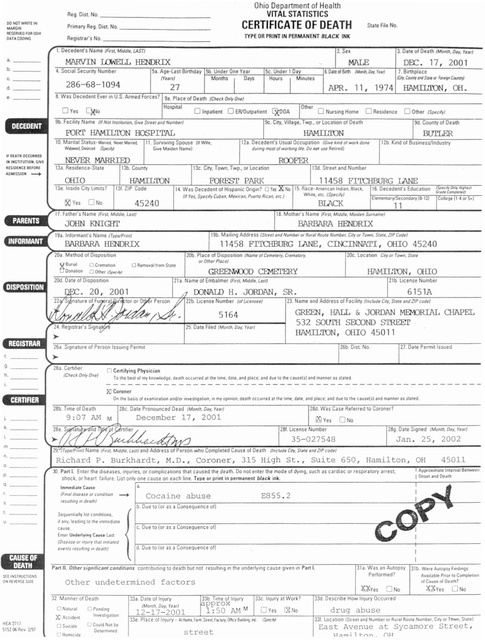
CERTIFICATE OF DEATH
_
Registrars No.
OATACOO'HG
Ohio Department of Health
VITAL STATISTICS
_
1. Oeceden!"s Name (F"st Middle, LAST)
a.
_
b.
_
c.
_
d.
_
e.
_
Stale File No.
TYPE OR PRINT IN PERMANENT BLACK INK
_
2. Sex
3. Date of Death
MALE
4. Social Security Number
Sa. Age-Last Birthday
I-'Sb::;-:.U",n.:.::d:;:e.:. r.:.D:.:;ne,_y.:.:e;;:a::..r_-+:::;:,==....:..:~,-.,_-l
Months
/Years}
286-68-1094
DB:. 17, 2001
7. B.rthplace
/CIfr, """'Y iIld 5'.. or For.." eo...ryj
(Monrh,II.1y. Yur/
Days
27
(Month. Dar, rur)
11, 1974
HAMILTON, 00.
8. Was Decedem Ever in U.S. Armed Forces? 9a. Place of Death (Check Dn'r One/
hH"o:-:"s":"'pitc:a:7I----------------r;;:;:-:-:-----------------------
0
o
Inpatienl
0
0
ERJDulpatient
0
ReSidence
Other (S~cly/
9d. County of Death
FORr HAMILTON HOSPITAL
10. Mantal Slatus- Marrlf4, ..., Morn...
W.......
Door,..
HAMILTON
12a. Decedenl's Usual Occupation
II. Survivong Spouse (II W4e,
/SpecJr/
12b. Kind of Bus.nessilndustry
(GIve kmd o(work done
dUflng most of working Isf, 00 no' use RetJre-d)
G,ve Malden Name'
If DEATH OCClMUD
IN INSllTUTION. GrvE
IIIESIDEHtE I£fO",(
ADMISS'OH
-+
13a. ReSidence-State
13b. County
OHIO
13c. City, Town, Twp., or Locaoon
HAMILTON
13e. InSide C,ty Um.IS'
13f. ZIP Code
11458 FITCHBURG Ik"'lli
FOREST PARK
16. Decedenfs Educatoon
14. Was Decedent of Hispanic Dngln? 0 Yes
(If Yes, Specify Cuban, Me"c.n. Pueno RIcan. etc.)
0Cl Yes 0
45240
No
17. father's Name
BlACK
ame
(F"st MIddle, Last!
I
""hen
«J1y
G(~d. ComcJtr.4/
OemenlarylSecondary 10-121
conego 11-4 or 5.1
11
(f"st MIddle.
Ma.rlen Surname)
JOHN KNIGHT
19a. Informant's Name
I'
19b. Malhng Address
(TypeIPrlllri
BARBARA HENDRIX
20a. Method of OlSpos'Oon
Bur..1
0 CremallOn
DonatIon
lJ Other
(Sue., and NumurOf Ru"l Route
Number. City or Town, S,.te.lJP Code)
11458 FITCHBURG lANE, CIOCINNATI, OHIO 45240
lOb. Place of DIspOSition (Name o( Cemetery, Crem.wry.
or Olio., PI.ce/
o Removal from Slate
2Oc. Locaoon
HAMILTON, OlUO
ISPIClly,
2Od. Date of Disposition
21a. Name of Embalmer
'I
21b. License Number
(First Middle. Lasrl
6151A
OONAlD H. JORDAN, SR.
22b. License Number (oIlJcensee/
23. ame and Address of facrllty
25. Date fded
(Month, Dar.
Y.a,/
Signalure of Person Issuong Permll
g._---
----
28a. Ceruller
(J
(Chock Dn'r One)
(Include CIty, Stare and llP code)
GREEN, HALL & JORDAN MEM)RIAL CHAPEL
532 soum SEXX)ND STREEI'
HAMILTON, OHIO 45011
5164
h.
City 0' Town. Stall
26b. Dist. No.
27. Date Permit Issued
Certifying Physician
To lhe best of my knowledge. death occurred at the tune. dale. and place. and due to the cau.seh) and manner as suted.
ro Coroner
On Ihe basIS 0' eaaminatlOn and/or InveStlgatlon. in my opinion. death occurred at the tMl'le. dale. and place; and due to the
28b. T,me of Death
~1
9:07
k..
m
(Month, D.y.
December 17, 2001
M
causeh~
and manner as stated.
rearl
DNo
_
28g. Date Signed
(Include City. State .nd lJP cod.1
_
Burkhardt, M.D., Coroner, 315 High St., Suite 650, Hamilton, OH
_
p._--q----
(Month, Day. re.r)
Jan. 25, 2002
35-027548
_
n.
0.
28c. Date Pronounced Dead
(Fmal dlSelJse Of condlCJOn
-+
I Onse' .nd Dea'h
E855.2
Cocaine abuse
fI$uJrmg In death)
45011
ApprOXimate Interval Berween
Part t Enter the diseases, mjuries, or complications that caused the death. Do not enter the mode of dying, such as cardiaC or resprratory arrest.
shock. or hean faliure. List only one cause on each line. Tyoe or orin! in oermanent black ink.
a.
Immediale Cause
b. Due to (0' as a Consequence ofl
Sequenllarty hst cond.uon.s.
u.
_
If any. leadIng to the mmedlate
c. Due to (or as a Consequence of)
cause.
Enter Underlyi"9 C~u.s. Last
(D,jeiJSe Of mJury that Ift/tlated
events resulting
Part II.
SH 'NSrlllJCTIONS
ON R£Y[IIS£ S,oE
1ft
Other s;gn;(;canl cond;l,ons
conlflbulong to death but not resuh,ng rn the underlyIng cause gIven rn Part!'
Other undetermined factors
32 Manner of Death
o Nalural
)C Awdenl
HEA1711
5152 R.v 21'31
d. Due to (or as a Consequence ot)
death)
o SVlclde
o Pendong
IrwesllgalJOn
U Could NOI be
Oetermtned
0' CilUSli! of Death'
~Yes 0
33d Describe How Inlury Occurred
33b. Time ot Inlury
33a. Date of InJUry
pprox
(Month, Day. rear/
12-17-2001
31a. Was an Autopsy 31b. We,e Autopsy F.. dlngs
Performed?
Available Prior (0 Compleoon
1: 50 AM
M
33e. Place of Inlury - AIHocn•.f.. m.S..... f"IOrf.Ot'c.B~.•"
street
0
)Q}Yes
0
0
drug abuse
33t. Locallon ISue.' and Number or Rural Rou,e Number. Cily or Town. S'ale'
East Avenue at Sycamore Street,
~T.:>mi't-,...,n_
()1-l