
Taser X26 and Pacemakers Cleveland Clinic
Download original document:
Document text
Document text
This text is machine-read, and may contain errors. Check the original document to verify accuracy.
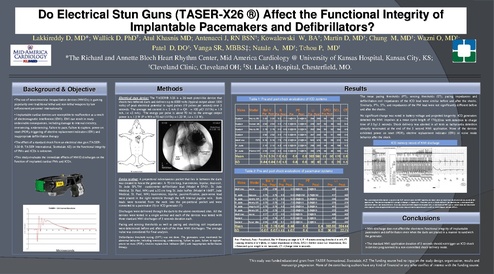
Do Electrical Stun Guns (TASER-X26 ®) Affect the Functional Integrity of Implantable Pacemakers and Defibrillators? Lakkireddy D, MD*; Wallick D, PhD†; Atul Khasnis MD; Antenacci J, RN BSN†; Kowalewski W, BA†; Martin D, MD†; Chung M, MD†; Wazni O, MD†; Patel D, DO†; Vanga SR, MBBS‡; Natale A, MD†; Tchou P, MD† *The Richard and Annette Bloch Heart Rhythm Center, Mid America Cardiology @ University of Kansas Hospital, Kansas City, KS; †Cleveland Clinic, Cleveland OH; ‡St. Luke’s Hospital, Chesterfield, MO. Background & Objective •The use of neuromuscular incapacitation devices (NMIDs) is gaining popularity over traditional lethal and non-lethal weapons by law enforcement personnel internationally • Implantable cardiac devices are susceptible to malfunction as a result of electromagnetic interference (EMI). EMI can result in many undesirable consequences, including damage to internal circuitry, oversensing, undersensing, failure to pace, failure to capture, power on reset (POR), triggering of elective replacement indicators (ERI) and inappropriate defibrillation therapy Results Methods Electrical stun device: The TASER® X26 is a 26-watt pistol-like device that shoots two tethered darts and delivers up to 6000 volts (typical output about 1500 volts) of peak electrical potential in rapid pulses (19 pulses per second) over 5 seconds. The average net current is < 2 mA (I = Q/t = 100 µC/ (1/19s) = 1.9 mA, i.e <2 mA). The energy per pulse is about 70 mJ so the average output power is < 1.5 W (P = W/t = 70 mJ/ (1/19s) = 1.33 W, i.e < 1.5 W). Table 1: Pre and post shock evaluations of ICD systems Make Model R PT Pre DFCI DCL LI CT Pre Post Pre Post Post Vitality DS 3.20 3.20 9.3 7.1 1.4@0.5 0.4@0.5 394 369 54 52 178 7.6 Guidant Ventak MS 2.58 2.58 8.0 7.8 0.2@0.5 0.2@0.5 389 397 50 49 160 5.4 Guidant Vitality DS 3.19 3.19 8.0 6.9 0.2@0.5 0.2@0.5 352 354 50 52 154 4.9 2.93 2.93 8.0 7.0 0.2@0.5 0.2@0.5 367 348 54 51 169 8.4 5.16 5.16 7.5 7.5 2.0@0.4 2.0@0.4 500 474 59 59 210 5.6 3.10 3.10 4.2 4.9 0.2@0.5 2.2@0.5 395 380 44 44 196 5.2 3.00 3.00 4.3 4.4 0.2@0.5 1.0@0.5 355 375 46 46 165 4.3 Guidant Medtronic •The effect of a standard shock from an electrical stun gun (TASERX26 ®, TASER International, Scottsdale AZ) on the functional integrity of PMs and ICDs is unknown. Bat V Pre Post Pre Post Guidant 7273 The mean pacing thresholds (PT), sensing thresholds (ST), pacing impedances and defibrillation coil impedances of the ICD lead were similar before and after the shocks. Similarly, PTs, STs, and impedances of the PM lead were not significantly different before and after the shocks. No significant change was noted in battery voltage and projected longevity. ICD generators detected the NMI impulses at a mean cycle length of 176+20ms with detection to charge time of 5.9+1.5 seconds. Shock delivery was aborted in all tests as tachycardia detection abruptly terminated at the end of the 5 second NMI application. None of the devices exhibited power on reset (POR), elective replacement indicator (ERI) or noise mode behavior after the shock. ICD memory record of NMI discharge St. Jude St. Jude •This study evaluates the immediate effects of NMID discharges on the function of implanted cardiac PMs and ICDs. Photon VR Mean 3.31 3.31 7.0 6.5 0.6 0.9 393 385 51 SD 0.84 0.84 2.0 1.3 0.8 0.9 50 42 5 50 176 5.9 5 20 1.5 Table 2: Pre and post shock evaluations of pacemaker systems Device testing: A prepectoral subcutaneous pocket that lies in between the darts was created to house the generator. A 70 cm long, transvenous, bipolar, dual-coil, St. Jude SPLTM cardioverter defibrillator lead (Model # SP-01, St. Jude Medical, St. Paul, MN) and a 52 cm long St. Jude Isoflex (Model # 1648T, Jude Medical, St. Paul, MN) transvenous, bipolar, passive-fixation, pace-sense lead were placed in the right ventricle through the left internal jugular vein. Both leads were tunneled from the neck into the pre-pectoral pocket and were connected to a pacemaker (9) or ICD generator (7) Discharges were delivered through the darts to the above-mentioned sites. All the devices were tested in a single animal and each of the devices was tested with three standard NMI discharges of 5 seconds duration each. Make Model Bat V R Pre Post Pre Post PT Pre LI Post Pre Post Medtronic Insync 2.95 2.95 8.0 8.0 0.5@0.5 0.5@0.5 422 409 St. Jude Enpulse 2.75 2.75 5.6 5.6 0.25@0.52 0.75@0.52 417 423 St. Jude Identity DR 2.73 2.71 5.0 5.3 0.25@0.5 0.25@0.5 334 356 St. Jude Affinity DR 2.75 2.75 7.0 7.0 0.25@0.8 0.25@0.8 374 374 St. Jude Integrity AF 2.75 2.76 6.2 6.4 0.25@0.4 0.25@0.4 401 383 St. Jude Affinity DR 2.76 2.76 7.0 7.0 0.25@0.5 373 403 Medtronic Insync 2.77 2.77 8.0 8.0 0.5@0.5 0.5@0.5 426 422 2.78 2.76 5.7 5.3 0.3@0.5 0.3@0.5 410 400 2.85 5.1 380 380 Guidant Guidant Pulsar Max 2.86 5.8 0.2@0.4 0.25@0.5 0.3@0.4 Pacing and sensing thresholds as well as pacing and shocking coil impedances were determined before and after each of the three NMI discharges. The average value was considered for final analysis. Mean SD Defibrillation threshold testing (DFT) was not done. The generators were monitored for abnormal behavior, including oversensing, undersensing, failure to pace, failure to capture, power on reset (POR), elective replacement indicator (ERI) and inappropriate defibrillation therapy. Pre ‐ Preshock, Post ‐ Postshock, Bat V– Battery voltage in V, R – R waves sensing threshold in mV, PT – pacing threshold in V @ms, LI –Lead impedance in Ohms, DFCI – Defibrillation Coil Impedance, DCL – Detected cycle length in milliseconds, CT – Charge time in seconds. 2.79 0.07 2.78 6.40 0.07 1.15 6.48 1.07 0.3 0.1 0.4 0.2 393.00 394.44 30.15 22.71 This interrogated electrogram strip from the ICD memory after the NMI application shows onset of rapid rate detection with initiation of the application. The device responds by starting to charge its capacitors. However, prior to shock delivery, the application is terminated and the device aborts the shock delivery. Note that detected cycle length corresponds best to the detected NMI pulses rather than the ventricular electrograms even though accelerated ventricular capture can be appreciated visually at cycle lengths around 240 ms. Conclusions • NMI discharge does not affect the short-term functional integrity of implantable pacemakers and defibrillators even when the darts are placed in a manner to sandwich the generator. • The standard NMI application duration of 5 seconds should not trigger an ICD shock in devices programmed to a non-committed shock delivery mode. This study was funded educational grant from TASER International, Scottsdale, AZ. The funding source had no input on the study design, organization, results and manuscript preparation. None of the contributing authors have any kind of financial or any other conflict of interest with the funding source.